
Muscle strains, torn muscles, pulled muscles, DOMS?!?!
Part 2.
After reading Part 1 you should be feeling a bit wiser on what muscle strains/DOMS can feel like and why they happen. In Part 2 we’ll cover some basics of what to do and how to best kick-start your rehab journey.
Early stages of physiotherapy rehabilitation for muscle strains and DOMS.
Often we find ourselves stuck with questions such as “How long will this take to heal?” or “When can I go back to playing competitive sports?” or “Should I ice it or put a heat pack on it?” Firstly let’s state that there is no miracle cure, no magic wands or special pills that replace healing time and hard work. But that doesn’t mean you can’t make things as comfortable as possible in the meantime. And it also doesn’t mean that you can’t do other things to keep you physically active and happy.

DOMS recovery
When looking through research literature, the jury is still out when it comes to what works best in minimising DOMS/recovery time. Interventions can include cryotherapy (ice or cold exposure), massage, compression, stretching, massage guns, creams, and a whole plethora of other knick knacks you can think of. Be cautious with anything that promises or sells miracure cures (remember there aren’t any). The evidence that does exist suggests that most of the aforementioned interventions may provide some pain relieving effects short term, but anything past that is still not 100%.
For many individuals with DOMS, management may simply mean getting back to some light mobility work or gentle exercise, or even just exercising another part of your body. This is one reason why many individuals like to isolate body parts (think leg day, arm day etc) during gym sessions, that way they allow rest days during the DOMS recovery period.

To hot pack or cold pack?
I find heat packs and ice packs are hugely personal preference (some people love heat packs, some people love cold packs). If we are getting technical and looking at the physiological mechanisms then usually a heat pack for muscle relaxation and to increase blood flow, and ice packs to help hinder swelling and inflammation. A recent study by Jerrold Petrofsky and his colleagues in 2015 looked at heat and cold therapy both immediately after exercise and 24 hours after exercise, and its effects on strength, pain levels and several other measures. Their results indicated that both were useful for different things at different times.
Imaging or no imaging?
Imaging is not required for DOMS, however if soreness does persist for more than several days even with resting then a quick visit to your physiotherapist may be warranted. With strains, mild strains don’t often require imaging unless symptoms are persistent. Given imaging can be expensive and findings of imaging may not actually change rehabilitation management, many healthcare professions would recommend against imaging for low grade strains early on. Moderate strains may require imaging again depending on the recovery process so far, as well as the site of strain.
Severe strains typically do require imaging, as this will help clarify whether further referral to an orthopaedic specialist is necessary.
It should be noted that imaging is a great tool to rule out any nasty pathology, but doesn’t tell you where pain is nor how capable you are. Use imaging sparingly.
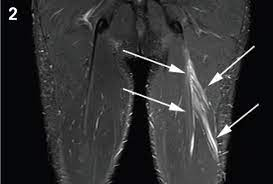
The above picture shows an MRI of a low grade hamstring muscle strain, where the muscle fibres show some oedema (swelling) but fibres are predominantly intact.
Courtesy of Aspetar Sports Medicine Journal (https://www.aspetar.com/journal/viewarticle.aspx?id=28#.YmnEDNpByUk)
Strains
For mild muscle strains the recovery process may take several days to several weeks, but you may be able to continue light or gentle exercise. It’s often a good idea to ease off intense sport or the specific exercise which caused the muscle strain to begin with, as you don’t want to keep hammering that same injured muscle whilst it’s healing. Maintain mobility and movement, but keep effort low, simply easing back the intensity/effort can do the trick with mild strains.
Moderate muscle strains will take longer, we are talking several weeks to potentially months. As mentioned before this will be influenced by the location of the injury. For these injuries there may be a period of relative rest, and usually you will have to “baby” the injured area for a good while before going back to your exercise. Mild analgesics (such as paracetamol) or anti-inflammatories may be required to help with symptoms. If there is some muscle tension or tightness after the healing process is complete, gentle stretching may be introduced but avoid this during the early days of recovery.
Severe muscle strains will take the longest, and recovery can be months if that. In these cases imaging is usually advised to help determine if surgical input is required.
Anti-inflammatory medication or not?
There is discussion amongst healthcare professionals nowadays regarding the use of anti-inflammatory medication during early stages of soft tissue injuries. It is argued that disrupting the inflammatory process during early stages of a soft tissue injury may interrupt the body’s natural physiological reaction to an injury. What happens is during the inflammatory stages (usually lasting for several days after an injury) the body floods the injury site with cells that limit further injury and kick-starts the healing process. Thus stopping this would appear counterproductive to healing and optimal tissue repair.
HOWEVER, given inflammatory pain can be quite significant and limit the amount of active recovery/rehab you may partake in there should always be a balance between using medication for symptom relief when needed, and avoiding it if possible.

Courtesy of Dubois & Esculier (doi.org/10.1136/bjsports-2019-101253)
TIPS FOR DOMS AND MILD TO MODERATE MUSCLE STRAINS.
Exercise:
-
Early loading and movement is key! Talk to your physiotherapist and find movements that your body likes or can tolerate, and avoid the ones that aren’t so great for the time being. This may include targeting all your muscles apart from the affected one (but may also include targeting the affected one in a reduced manner).
-
We know your body heals best and feels best when you move, gone are the days of absolute bed rest!
-
Mobilise early and avoid stretching until later stages of the healing process if necessary.
Pain relief:
-
Medications can be a great way to make the healing process a little more comfortable (think paracetamol and ibuprofen, always consult your GP or pharmacist for medication information).
-
Heat/cold therapy.
-
Creams/sprays – Topical creams can provide temporary pain relief (think brain distraction), with some topical creams also having anti-inflammatory properties as well.
Diet:
Protection:
-
In some cases taping, bracing or splints may be used during early stages of an injury, but remember you want your muscles and body to do the work in the long run and not the tape/braces/splints. Chat to your physiotherapist about best taping/bracing/splint options for your specific injury.
Later stages of physiotherapy rehabilitation
A common mistake with muscle strain rehabilitation is stopping when pain has fully resolved, after all pain is a great motivator! However, by the time muscles have healed and you are pain-free it is likely the muscle has weakened or deconditioned to a degree. Often we prematurely return to a high level of activity without doing the necessary work to get our injured muscle back to its former strength, if not further. As you can imagine this alone is a risk factor for a repeat muscle strain, and so the vicious cycle starts. Take your rehab a few steps further to really set yourself up brilliantly for the long run.
Making sense of all this and putting all the rehab principles into practice can definitely be a daunting task. To get your rehab on track for the best outcomes possible, book in to see your local friendly physiotherapist.
Part 2 SUMMARY
-
For DOMS, don’t worry! Keep going with gentle exercise, avoid high intensity stuff involving the sore muscles.
-
After being cleared for a severe strain, GET MOVING! Start low and slow and work within low/no pain movements.
-
Medications can help make the process more comfortable, but healing takes time. Be patient.
-
Keeping active will best help the healing process, and help retain muscle flexibility/range, cardiovascular endurance and muscle function.
-
Fuel your body with adequate protein and a variety of nutrients/food groups.
-
Imaging only when necessary.
-
Once you think you’re out of the woods, take it several steps further for re-injury prevention.





Recent Comments