

Greater trochanteric pain syndrome
Do you experience pain over the side of your hip/pelvis? Do your symptoms worsen when sleeping on your sides, or after performing physical activity such as jogging or walking up and down stairs? It could be Greater Trochanteric Pain Syndrome (GTPS).
What is GTPS?
GTPS is a relatively common condition where one feels pain over the side of their hip. These symptoms can often travel down the side of the leg or around the buttock region. It is thought that GTPS occurs due to altered biomechanics and reduced load capacity of the hip muscles. These muscles provide stability during standing, walking and other movements. GTPS may feel worse when first waking in the morning, during movement, or even after being sedentary for some time.
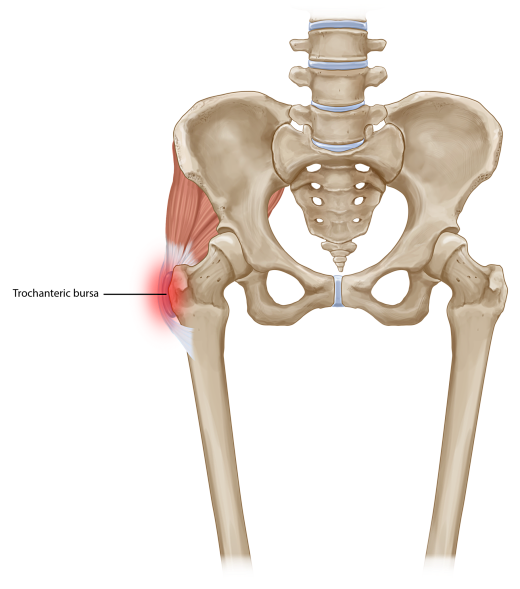
The components of GTPS can often be separated into 1) gluteal tendinopathy (often termed tendinosis if confirmed with ultrasound imaging), and 2) with or without greater trochanteric bursitis (again can be seen via ultrasound imaging). Gluteal tendinopathy simply refers to the musculotendinous component of the condition, and bursitis simply refers to the inflamed area of cushioning over the bony part of the hip area (see Figure 1.)
Who’s at risk?
GTPS is often seen in women above the age of 35-40 years, but can occur earlier and to anyone. Individuals often report a gradual progression of symptoms, which may be preceded by a specific change in activity or exact moment of injury. For example, you may have started running again, or you slipped and bumped your low back/hips, or you may have even been out with the flu and have been laying on the couch a bit more than usual.
Can we diagnose GTPS without imaging?
Diagnosing GTPS can be done quite accurately by a physiotherapist when using a combination or cluster of tests to improve sensitivity and specificity. For example, palpation of the greater trochanter and any combination of loading/compressive testing of the lateral hip structures/muscles (30 sec SLS test, FABER, FADER-R etc) gives the best diagnostic accuracy. It is important to distinguish those with GTPS and those experiencing lumbar spine referred pain, as symptoms can be felt around the same areas but will be managed differently.
Managing GTPS
Whilst it may be tempting to push through the pain, appropriate management may require certain activity and postural modifications to keep pain minimal.
This may include:
Sleep habits
-
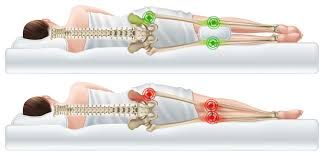
Sleeping on your back or front if possible. Sleeping on sides increases compression over the sore irritated bursa/muscle tendons and can further aggravate symptoms.
-
If sleeping on your sides, a softer mattress (mattress toppers are a great idea) may help reduce the compressive pressure over the sore area, or sleeping with a pillow between the knees may also help reduce compression over the sore area.
Sitting/standing postures
-
Avoid sitting with legs crossed where possible, as this further increases pressure over the sore area.
-
A higher chair height typically helps reduce the angle between your legs and pelvis, which may help reduce pressure over the side of your hips (try sitting on top of a pillow at the kitchen table).
-
Avoid putting more weight on the sore leg when standing still a.k.a. “Hip hanging”.
Walking/stairs
-
Walking uphill and stairs often increases loading and compression over the lateral hip muscles. If possible ease up on these activities for a short period to allow symptoms settle.
Medications
-
Oral anti-inflammatories may help the process along, and allow for you to get started on the active exercise and rehabilitation.
-
Local steroid injections may help relieve symptoms short-term, but there is some emerging research questioning the long-term effectiveness and safety of receiving too many steroid injections
Manual therapy
-
Some treatment directed over muscles involved may help relieve symptoms short term, but typically we avoid direct pressure over the bony aspect of the outer hip.
-
Taping may also be an option to help offload sore structures during movement.
EXERCISE
As with many injuries/conditions, exercise is key for long-term management of GTPS. Specifically targeting the muscles of the hip girdle, and addressing biomechanical factors will help resolve symptoms in the long run. However, knowing how much to do and what to do specifically is crucial as always. For example, walking 10 mins compared to 30 mins can be a completely different ball park for the affected muscles/structures, and may be the difference between a manageable exercise amount and an amount that makes symptoms worse.
A gradual loading program to strengthen those muscles of the pelvic girdle, and offloading sore structures with appropriate rest or modifications will get you feeling much better and get you back to doing what you love.



Recent Comments