
Understanding, Managing, and Moving Forward
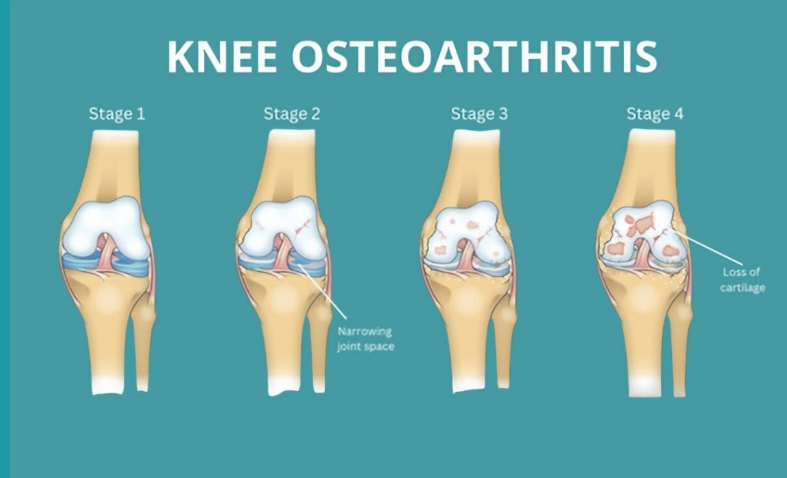
Knee osteoarthritis (OA) is a common condition that can cause ongoing pain, stiffness, and difficulty with everyday activities. It affects the whole joint — including cartilage, bone, ligaments, and muscles — and is part of your body’s active response to small joint injuries over time. While it can be uncomfortable, OA is manageable and doesn’t always get worse. With the right approach, most people continue to live active, fulfilling lives.
Diagnosis and Outlook
Doctors often diagnose knee OA based on symptoms such as pain lasting more than three months, morning stiffness under 30 minutes, and difficulty with movement. X-rays are usually unnecessary because they don’t reliably reflect pain levels or guide treatment. For most people, OA remains stable, with occasional flare-ups that settle with time. Only a small number of people will ever need a knee replacement.
The Importance of Physical Activity
Many people with knee OA reduce their activity levels out of fear of making the pain worse. In fact, avoiding movement often increases stiffness, weakness, and discomfort over time. Staying active is one of the best things you can do for your joints, muscles, and overall health.
You don’t need intense workouts — small, regular movements make a big difference. Moderate-intensity activity means you’re breathing a little harder but can still speak in sentences. Examples include brisk walking, swimming, cycling, water aerobics, yoga, or doing household tasks more energetically.
Tips for increasing your daily activity:
-
Take small steps — stairs instead of elevators, park further away, walk while talking on the phone.
-
Avoid long periods of sitting; move every 30–60 minutes.
-
Break activity into short bouts of 10 minutes or more.
-
Gradually increase duration or intensity.
-
Mix activities — walking, gardening, dancing, playing with grandchildren.
-
Track steps or activity using a phone or monitor.
-
Pace yourself and be kind to your body, even on “bad” days.
Managing Your Weight
Being overweight places extra stress on your knees — each kilogram of body weight can add about four kilograms of load on your knees during daily activities. Extra weight can also increase inflammation in the body, making pain and stiffness worse. Losing even a small amount of weight — 5–10% of your body weight — can reduce joint load, improve pain, increase function, and may delay or reduce the need for medications or surgery.
Tips for weight management:
-
Combine regular physical activity with healthy eating habits.
-
Set realistic goals and be patient; don’t give up if progress is slow.
-
Eat mindfully: slow down, savour meals, and avoid eating when bored or stressed.
-
Plan meals and snacks ahead, and keep a food diary.
-
Drink water regularly and aim for sufficient sleep.
-
Learn about healthy food choices and portion sizes.
-
Engage friends, family, or a buddy for support and accountability.
-
Handle holidays or special events by planning ahead — enjoy the event but make mindful choices.
Key points:
-
Weight loss can noticeably reduce knee pain and improve function.
-
Aim for 5–10% of your body weight to see meaningful benefits.
-
Combining diet and exercise gives the best results.
Overcoming Common Barriers
Everyone faces challenges staying active or managing weight. Creative solutions can help:
-
Time: Schedule activity like an appointment; short bursts count.
-
Pain: Mild discomfort is normal; severe or prolonged pain requires adjustment.
-
Fatigue: Exercise often increases energy and improves sleep.
-
Motivation: Track progress, reward yourself, exercise with friends.
-
Stress or emotional eating: Try music, social support, mindfulness, or walking instead of using food as a coping strategy.
The Bottom Line
Knee osteoarthritis does not mean you have to stop doing the things you love. Staying active, managing your weight, learning to manage pain, and seeking support from health professionals can help you live well with OA. Every small step counts toward stronger knees, reduced pain, and better overall health.
For additional information:
https://www.myjointpain.org.au

Recent Comments