
Achilles Tendinopathy

Understanding, Managing, and Moving Forward
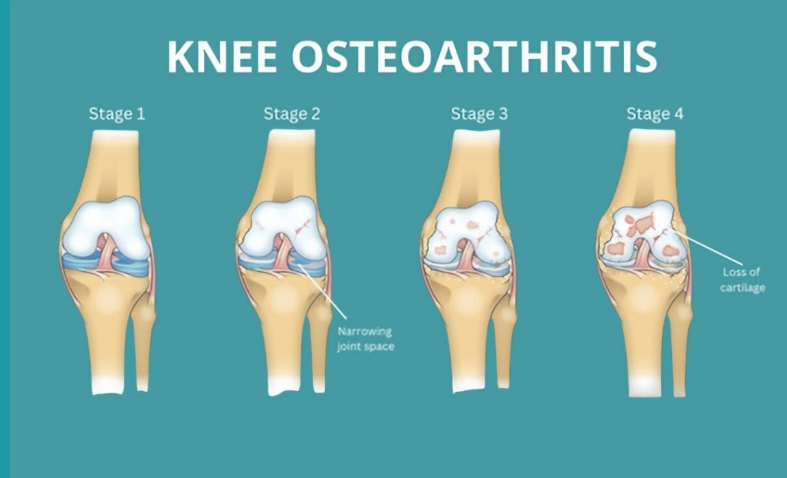
Knee osteoarthritis (OA) is a common condition that can cause ongoing pain, stiffness, and difficulty with everyday activities. It affects the whole joint — including cartilage, bone, ligaments, and muscles — and is part of your body’s active response to small joint injuries over time. While it can be uncomfortable, OA is manageable and doesn’t always get worse. With the right approach, most people continue to live active, fulfilling lives.
Doctors often diagnose knee OA based on symptoms such as pain lasting more than three months, morning stiffness under 30 minutes, and difficulty with movement. X-rays are usually unnecessary because they don’t reliably reflect pain levels or guide treatment. For most people, OA remains stable, with occasional flare-ups that settle with time. Only a small number of people will ever need a knee replacement.
Many people with knee OA reduce their activity levels out of fear of making the pain worse. In fact, avoiding movement often increases stiffness, weakness, and discomfort over time. Staying active is one of the best things you can do for your joints, muscles, and overall health.
You don’t need intense workouts — small, regular movements make a big difference. Moderate-intensity activity means you’re breathing a little harder but can still speak in sentences. Examples include brisk walking, swimming, cycling, water aerobics, yoga, or doing household tasks more energetically.
Tips for increasing your daily activity:
Take small steps — stairs instead of elevators, park further away, walk while talking on the phone.
Avoid long periods of sitting; move every 30–60 minutes.
Break activity into short bouts of 10 minutes or more.
Gradually increase duration or intensity.
Mix activities — walking, gardening, dancing, playing with grandchildren.
Track steps or activity using a phone or monitor.
Pace yourself and be kind to your body, even on “bad” days.
Being overweight places extra stress on your knees — each kilogram of body weight can add about four kilograms of load on your knees during daily activities. Extra weight can also increase inflammation in the body, making pain and stiffness worse. Losing even a small amount of weight — 5–10% of your body weight — can reduce joint load, improve pain, increase function, and may delay or reduce the need for medications or surgery.
Tips for weight management:
Combine regular physical activity with healthy eating habits.
Set realistic goals and be patient; don’t give up if progress is slow.
Eat mindfully: slow down, savour meals, and avoid eating when bored or stressed.
Plan meals and snacks ahead, and keep a food diary.
Drink water regularly and aim for sufficient sleep.
Learn about healthy food choices and portion sizes.
Engage friends, family, or a buddy for support and accountability.
Handle holidays or special events by planning ahead — enjoy the event but make mindful choices.
Key points:
Weight loss can noticeably reduce knee pain and improve function.
Aim for 5–10% of your body weight to see meaningful benefits.
Combining diet and exercise gives the best results.
Everyone faces challenges staying active or managing weight. Creative solutions can help:
Time: Schedule activity like an appointment; short bursts count.
Pain: Mild discomfort is normal; severe or prolonged pain requires adjustment.
Fatigue: Exercise often increases energy and improves sleep.
Motivation: Track progress, reward yourself, exercise with friends.
Stress or emotional eating: Try music, social support, mindfulness, or walking instead of using food as a coping strategy.
Knee osteoarthritis does not mean you have to stop doing the things you love. Staying active, managing your weight, learning to manage pain, and seeking support from health professionals can help you live well with OA. Every small step counts toward stronger knees, reduced pain, and better overall health.
For additional information:
https://www.myjointpain.org.au
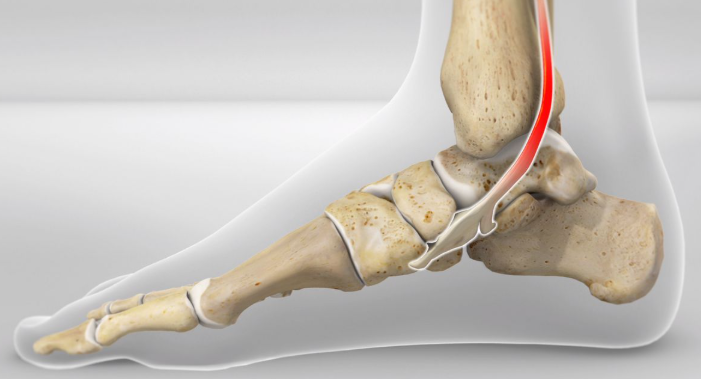
The tibialis posterior (TibP) muscle runs along the inside of your shin and down to your mid foot. It functions to invert and plantarflex the foot and control your arch. This means it plays a big role with walking, running and balancing.
TibP tendinopathy will present with pain and stiffness on the inside of your ankle and/or foot. There may also be swelling present. TibP tendinopathy pain will warm up with activity but often feels worse after a period of resting. It is typically associated with an increase of activity or a recent change in activity.
Examples might include:
– Someone who just took up running or increased their km per week
– An athlete bought a new pair of shoes for their sport
– A switch to synthetic turf when historically playing on grass
Tendons stem from our muscles which attach them to bone. Tendinopathy is considered an overuse injury of tendons. This means that the tendon is not coping with the demands that is being placed on it. This leads to pain and dysfunction of that tendon.
Assessment
Physiotherapists will ask about the history of the pain which will provide clues into whether it is or isn’t TibP tendinopathy.
A physical exam will also be performed which may include:
– Double or single leg calf raise
– Jumping or hopping
– Muscle strength testing
– Palpation of the lower leg
Imaging?
Imaging (ultrasound or MRI) is not typically required for accurate diagnosis of this injury. This is because imaging is poorly correlated with symptoms; a study found that under ultrasound imaging, 48% of people showed TibP tendinopathy despite have no medial foot or ankle pain (Mills et al., 2020).
Some people also present with normal imaging despite having clinical
features of TibP tendinopathy. Imaging is likely only required if your physiotherapist suspects a bony injury.
Treatment and Management
TibP tendinopathy can be successfully managed with physiotherapy. It may involve a period of relative rest and concurrent strengthening exercises of the TibP and other muscles in the body.
– Isometric ankle inversion
– Single leg calf raises
– Eversion
– Toe raises
– Energy storage and release exercises (hopping, depth jumps, lateral bounds etc)
– Strengthening of proximal muscles (hip and knee strength)
Other management strategies involve:
– Topical or oral NSAIDs (anti-inflammatory medication)
– Soft tissue release of TibP and other muscles in the lower leg
– Joint mobilisations
Differential Diagnoses – If it isn’t TibP tendinopathy, what else could it be?
– Deltoid ligament injury
– Navicular bone injury
– Flexor hallucis longus tendinopathy
– Tarsal tunnel syndrome
The apophysis is a normal outgrowth on long bones where tendons or ligaments attach. These areas will continue to fuse and harden as children get older and their growth plates fuse.
Apophysitis is a condition of overuse and inflammation at these apophysis sites. It is the result of repetitive stress from activities/sport. These injuries will worsen with activity and improve with rest. Since the apophysis growth plate is still open, combined with the repetitive action of muscles, this makes these areas especially vulnerable to injury.
Some common overuse apophysis injuries include:
1. Osgood-Schlatter’s Syndrome (knee)
2. Sever’s Syndrome (heel)
3. Little League Elbow (elbow)
4. Iselin’s Syndrome (outside of the midfoot)
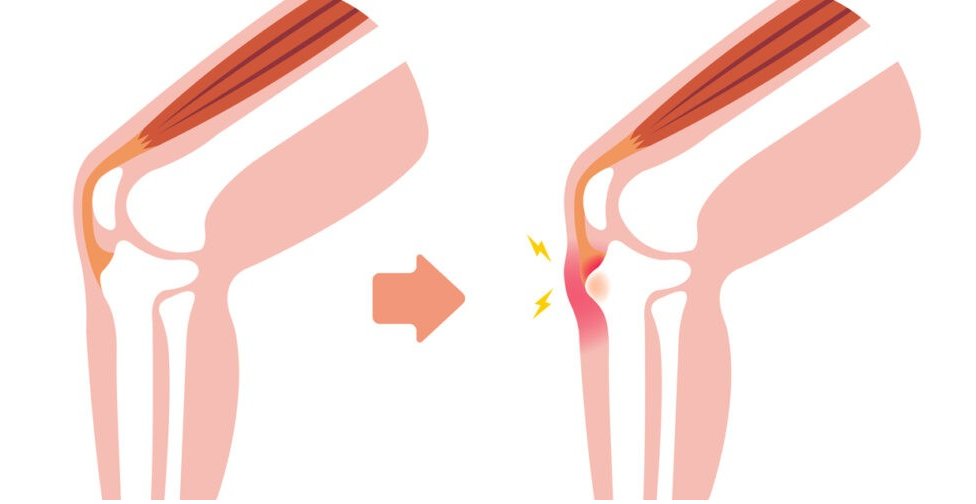
Osgood-Schlatter’s
This is apophysitis at the tibial tuberosity, or the bony bump at the top of your shin. This is where the quadriceps muscle attaches onto the shin via the patella tendon.
Signs and Symptoms
– Pain and/or swelling at the tibial tuberosity
– Pain at the knee when participating in sport/activity, especially running and jumping
– A recent growth spurt
– Symptoms resolve with rest
Sever’s
This is apophysitis of the calcaneus (heel bone). This is where the gastrocnemius and soleus muscles attach onto the foot via the Achilles tendon.
Signs and Symptoms
– Pain at the heel when participating in sport/activity, especially with running and jumping
– Pain and/or swelling at the heel
– A recent growth spurt
– Symptoms resolve with rest
Assessment
Physiotherapy assessment will begin with a subjective interview to gain insight into the history of the pain to determine if it is or isn’t apophysitis. Your GP may have requested an X-ray of the area which can help determine diagnosis, but it will sometimes come back normal.
The physiotherapist will look at:
– Squats
– Jumps and hops
– Calf raises
– Palpation of the painful area
– Muscle strength and length testing
Management
Apophysitis generally starts with a period of relative rest. Depending on the aggravating activities, other sports may be tolerated better in the meantime. For example, instead of going to soccer, riding a bike or swimming may be less painful.
Strengthening and stretching exercises are also essential to managing apophysitis. This might include stretching the quadriceps, hamstrings, calves and glutes. Strengthening of the affected muscles will also be key.
– Double leg glute bridges
– Theraband quad extensions
– Hip abduction exercises
– Squats or lunges
– Double or single leg calf raises
Other management strategies may include:
– Soft tissue mobilisation of the affected muscles
– Foam rolling or spikey ball at home
– Movement retraining
– Rigid taping or KT taping of the affected area for symptomatic relief



Spring has sprung which means cricket season is officially upon us.
Cricket is a popular non contact sport that requires a combination of physical fitness, skill, and strategy. Overuse and impact injuries are common since players engage in running, throwing, batting, bowling, catching, and diving. A physiotherapist can identify risk factors for prevention of sport injuries, provide effective strengthening/conditioning exercise programs to improve muscle imbalance and promote safe return to sport
So let’s take a look at some of the most common injuries
Lumbar spine injuries are very common in fast bowlers since the technique involves placing a large amount of force repetitively through the back at great speed. The result of repeated or forceful trunk lateral flexion with rotation during the delivery stride and follow-through puts the lumbar spine at risk of developing disc degeneration or spondylolysis, a stress fracture occurring at the pars interarticularis. Bowling injuries tend to be overuse injuries and often present gradually over time. It occurs more often in young fast bowlers and are usually seen on the side opposite to the bowling arm.
The rotator cuff muscles are stabilizing muscles around the shoulder joint. A rotator cuff injury is an overuse injury due to repeated overhead throwing during fielding, bowling and wicket-keeping.
Cricketers are prone to hamstring strains because they may be required to perform an explosive movement after a long period of standing relatively still. Hamstring strains occur during sprinting with fast bowling, while fielding or sprinting between wickets as a batsman. The severity of the strain may vary between a dull ache or extreme pain making it difficult to stand or walk.
Contacts to email:

A research piece recently published in the British Journal of Sports Medicine described “extraordinary levels” of ice used at the summer Olympics as not always being evidence-based and bad for the planet.
They report that over the last decade, there has been a sharp increase in CWI requests. Data provided courtesy from games organizers indicate that the request for CWI at Athens 2004 and London 2012 were 10% in comparison with Rio 2016 at 44%, where the majority of these were used for recovery. Tokyo 2020 Olympic games required 22 tons of ice and had an additional 42 tons delivered to the Olympic village residence for ice dispensing machines. Paris 2024 first estimated 1624 tons of ice, at a cost of €2.5million, however, the estimate was reduced to 650 tons (450 tons for the Olympics and 200 tons for the Paralympics). The researchers point out the environmental concerns as ice provision requires a considerable amount of energy for production and storage as well as logistical challenges related to transportation. In addition, ice is often used to obtain benefits which are not evidence-based. More importantly, ice could have the opposite effect to that expected, such as delayed tissue regeneration or impaired recovery.”
Cryotherapy (also known as cold therapy) is utilized as a physical intervention in the treatment of injury and exercise recovery. This may vary from ice packs, compression pumps, ice baths, ice towels, ice massage and cold water immersion. Traditionally, ice is used in the treatment of musculoskeletal injury to reduce pain while cold water immersion (CWI)is used to reduce muscle soreness for recovery from exercise.
( Kwiecien SY, et al. Eur J Appl Physiol. 2021 Aug;121(8):2125-2142.)

Postexercise CWI is one of the most widely used recovery strategies among athletes and pooled data analysis show that it is better for muscle power and perception of recovery than active recovery, massage or contrast baths. However, recent studies have reported that cooling decreases long-term strength adaptations (Roberts et al. J Physiol 2015;593:4285–301) and may impair acute performance following exercise (Solsona et al. J Sports Sci 2023;41:1126–35). The researchers suggest therefore given the financial, logistical and environmental implications involved in setting up a CWI area at a competition venue , the approach of organizers should rather be tailored towards recovery goals in order to reduce ice requirements. They advise that CWI may be recommended and appropriate for recovery following exercise in the heat for fast relief of heat exhaustion, prolonged exercise in normal temperatures for relief of muscle soreness and during multi day training conditions where muscle soreness is anticipated over several days. They also suggest that CWI may be ineffective or unsuitable for recovery when used for high intensity consecutive exercise, acute recovery following resistance training and long term recovery following resistance training.
They conclude that ice should remain available for the relief of acute pain, specific recovery needs and management of heat stroke and organizers should plan better for the provision of ice to minimize the use of non-evidence-based practices and promote better sustainability. The sport and exercise medicine community needs better data on the actual amount of ice consumed at major sporting events, for what purposes and at what financial and environmental costs.
Interesting read!
Melissa Martin

Recent Comments