
Muscle strains, torn muscles, pulled muscles, DOMS?!?!
Part 1.
We’ve all heard of the common old “I’ve strained/pulled/torn a muscle” or even the basic “Ohhh the muscles are a tad sore after that workout!”. But what has actually happened when you get a strained/torn/pulled muscle? And why do we experience DOMS (delayed onset muscle soreness) after a good workout? Knowing what happens during a muscle strain is the first step in understanding how to best manage your muscle soreness or injury, and will get you set up for the best outcomes both short- and long-term.
Basic muscle anatomy
To understand muscle strains and DOMS we must first appreciate that muscles are complex and adaptable things. Picture muscles as a bunch of tubes (called sarcomeres) bundled together like many straws, which attach from bone to bone via tendons (see Image 1). Muscles (red part) have a stretchy, elastic-like property (think strong elastic band) and do all the hard work. Tendons (white part) on the other hand don’t do as much work, but act more to transfer force that the muscle produces, and connect muscles to bone. Tendons are strong, flexible, and play an important role as well.
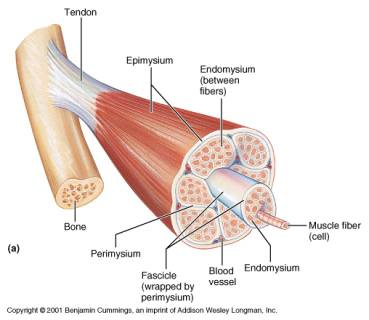
Image 1. Cross section of a muscle
How does a muscle work?
Muscles are living, breathing (sort of) things which work by pulling (concentric contraction) and releasing (eccentric contraction). Picture a bicep curl. Your bicep works concentrically to lift the weight up and bend at the elbow, and works eccentrically when slowly lowering the weight back to a straight arm position (see Image 2). In technical terms muscles work via the ‘sliding filament theory’ involving actin and myosin units which form the sarcomeres. Both concentric and eccentric muscle contraction requires varying degrees of effort, and this is where muscle injuries and soreness starts to come into play.
Image 2. Concentric and eccentric contraction of the biceps muscle.
Why do muscle strains occur???
Muscle strain injuries ultimately result from tissue/muscle failure. In other words, the muscle is exposed to a load or force higher than they can handle, and the activity demand exceeds the muscle capacity.
Exposure to load/force can come from a variety of sources. This includes lifting heavy objects, to repetitive movements (for example running), to high velocity moments (for example changing direction during footy). Exposure to load/force can lead to small micro-tears within the muscle, and if the force is great enough or prolonged enough then larger sized tears can obviously occur. Remember, since muscles are living/breathing things so they can be slowly trained to adapt to load. This is where DOMS comes in!

What are DOMS?
DOMS refers to that generalised muscle ache we get after a good exercise session, or after attempting a new exercise your body isn’t quite used to yet. I’m sure many of you can remember a time where you have gone back to the gym or a sport after holidays, and the next few days feeling pretty darn sore for the next few days. Then gradually over a few sessions your body gets used to said exercise and that soreness slowly goes away. That is ADAPTATION in a nutshell.
To explain this in slightly more technical terms, during an exercise session you are exposed to high or repeated external forces causing small micro-tears to your muscles, but in a manner that is controlled, not overly painful, and within your muscle tissues capacity (think lifting weights, or doing gentle cardio). Following the cool down period after your exercise session, the body begins the healing process and its associated inflammatory reaction to heal these micro-tears and rebuild your muscle tissue stronger than before (ADAPTATION).It is believed that these micro-tears and the inflammatory response (and several other theories) are what causes DOMS. The peak of DOMS typically sets in 1-2 days after the session is completed, and the soreness begins to ease after this.
It should be worth noting that you do NOT need to experience DOMS in order for adaptation or hypertrophy (building muscle size) to occur. However, the more you exert and challenge a muscle differently the more likely DOMS will occur.
What does a muscle strain/DOMS feel like?
With muscle strains individuals may describe a painful strong pulling sensation, which can appear sharp in nature and progress to more of a strong achy feeling over time. In more significant cases a strong pop may be felt. During early stages there may be limited movement around the injured area, and you may notice some bruising and swelling develop over time. Pain is most likely worsened when attempting to use the affected muscle.
Likewise, DOMS can often result in limited movement but to a lesser degree, and symptoms typically ease with gentle movement. Strains are often felt at the time of exercise, particularly the more severe ones, whereas DOMS is felt over the next few days.

Why do some muscle injuries heal quicker than others?
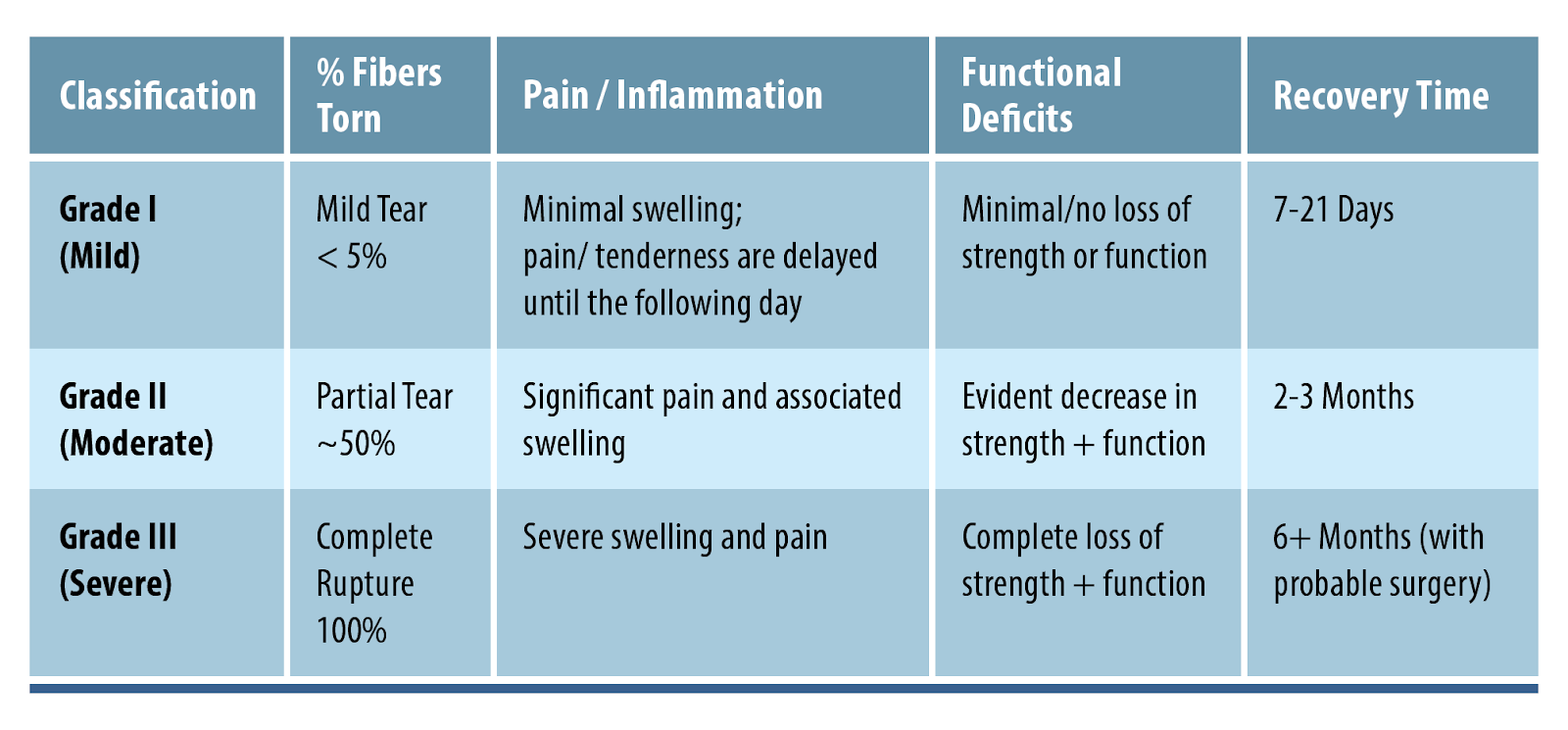
Healing rates of muscle injuries are largely dependent on the location. The injury can occur in three distinct locations; the periphery of the muscle (myofascial), in the bulk of the muscle (musculotendinous), or in the tendon (intratendinous). The most commonly injured location is the musculotendinous part. Naturally, the extent of the injury will also influence how long it takes to heal. Muscle strains can be graded using different scales, although the simplest and most commonly used grading system ranks strains as shown below.
Other comorbidities such as diabetes or smoking can notably slow down healing rates as well.
Part 1 SUMMARY:
-
Sore muscles after a big workout or different workout is normal!
-
DOMS typically occurs the next few days following a workout, whereas a strain is typically felt at the time of exercise.
-
Muscle strains typically occur when the demands of a muscle exceed its capacity.
-
Muscles are adaptable to load, training them up slowly and steadily is your best bet.
-
Healing times vary between degrees of strain, and personal factors as well. Make your own journey!
An early and thorough assessment following a muscle strain is essential whether you are wanting to simply get back on your feet or return to high level sports. Book in to see your physiotherapist for a thorough assessment and tips on how to best handle your individual rehab journey.
______________________________
WILSON TANG, PHYSIOTHERAPIST









Recent Comments